Soft Tissue Sarcomas Imaging Guidelines
Guidelines for diagnosis, biopsy and reporting of suspected sarcoma
Flow Chart for Suspected Sarcoma
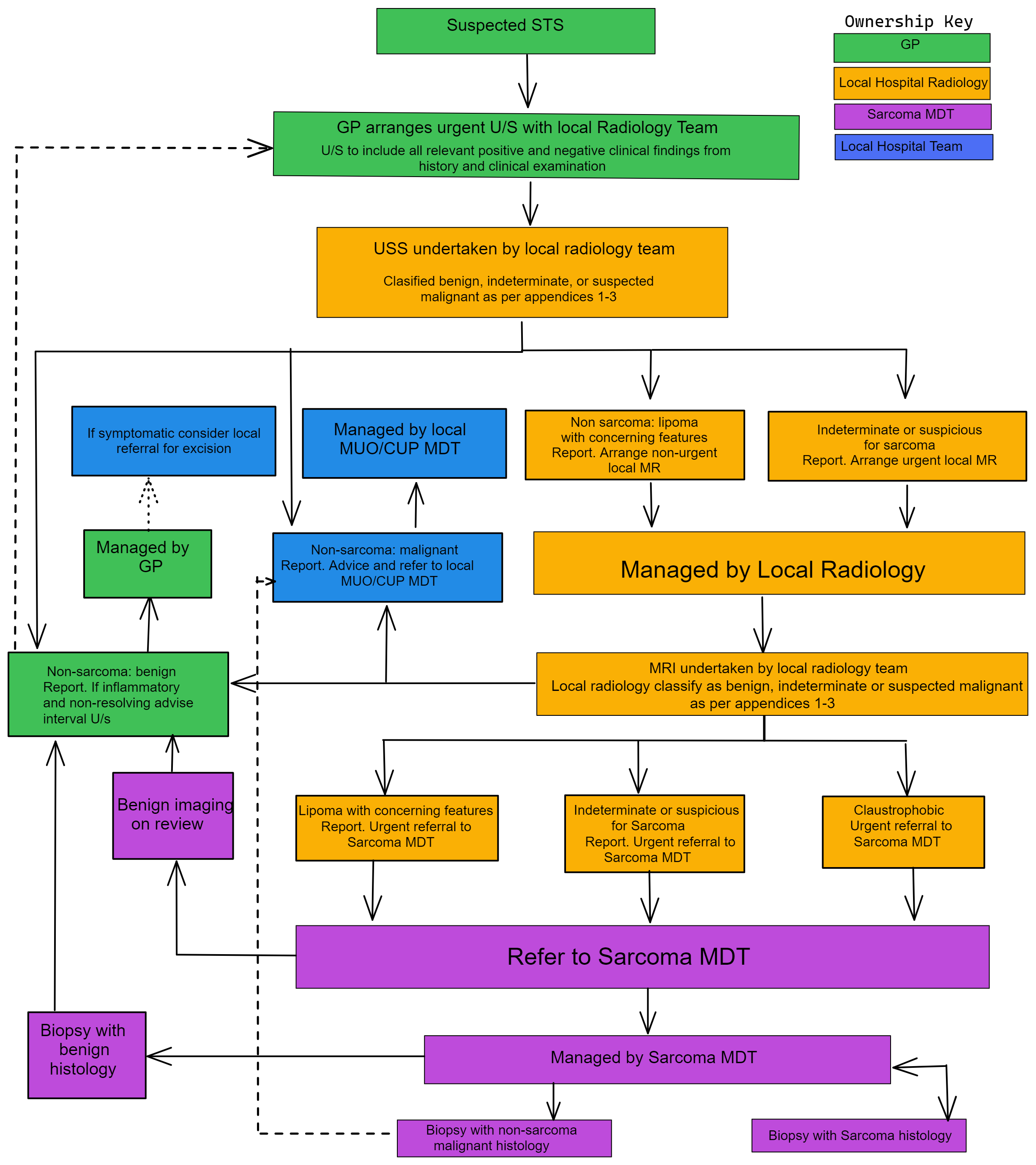
Diagnosis
Patient attends GP with soft tissue mass and is assessed clinically;
a. Observe/Discharge
b. Investigate
Ultrasound
a. History re-taken regarding – size, duration, precipitants, growth, associated symptoms. Examined for position and local changes.
b. Ultrasound examination assesses – mass size, location (relation to fascia and anatomical location), echotexture, cyst/solid/mixed, Doppler characteristics.
- If diagnostic for non sarcoma (benign) (appendix 1) – report to GP. If appears inflammatory consider interval imaging.
- If diagnostic for non sarcoma (malignant) by history and appearances – report to GP to refer to local oncology (CUP MDT).
- If diagnostic for lipoma but concerning symptoms (appendix 2) – report to GP +/- MRI (notify sarcoma service – non urgent). If lesion is being referred due to concerning clinical features this needs to be mentioned on the report.
- If suspicious for sarcoma or indeterminate (appendix 3)–report to GP + radiologist organises local MRI.
MRI – performed if not definitive on Ultrasound/local staging.
a. Recommended guidance for protocol – appendix 4. (If claustrophobic refer to sarcoma service with ultrasound).
b. MRI findings:
- If diagnostic for non sarcoma (benign) (appendix 1) – report to GP. If appears inflammatory consider interval imaging.
- If diagnostic for non sarcoma (malignant) (appendix 2) – report to GP and refer local oncology (CUP MDT).
- If suspicious for sarcoma or indeterminate (appendix 3)–report to GP (notify sarcoma service -urgent).
Biopsy
- In nearly all cases, performed by sarcoma MDT and MDT radiologist.
- Occasionally can be performed locally (outside sarcoma MDT) if sarcoma MDT and local radiologist agreeable and sent to sarcoma histopathologist.
Provision of Referrer Guidance within Radiology Reports
The following reporting suggestions are to make clear the responsibility of the referrer in advancing management where referral to the sarcoma MDT is not indicated but when further local action is needed.
To support category 5 or 6.1 findings:
Report: Lipomatous mass with no aggressive features on imaging. If symptomatic advise referral to local surgical unit for consideration of removal.
To support category 4, 6.2, or 7 findings where radiology concern persists in the absence of a defined radiological diagnosis:
Report: No specific or aggressive features on imaging, but given the clinical features advise local clinical review in 3-4 weeks and if there is persisting concern arrange repeat imaging at that time. Referral to the sarcoma MDT is not required unless the serial imaging is suspicious for sarcoma.
Note for reporting radiology teams:
Repeat imaging does not need to be referred to the sarcoma MDT for review unless there is radiological concern for sarcoma based upon the imaging criteria set out in the Appendices of this document.